Understanding Sleep Apnea: More Than Just a “Loud Snore”
Sleep is often viewed as a passive state of rest, but for those with pulmonary sleep disorders, it can be a nightly struggle for oxygen. In a detailed clinical breakdown, Ninja Nerd explores the two primary beasts of sleep-disordered breathing: Obstructive Sleep Apnea (OSA) and Obesity Hypoventilation Syndrome (OHS).
While many dismiss snoring as a mere annoyance, these conditions represent serious medical risks that can impact your heart, brain, and overall longevity.
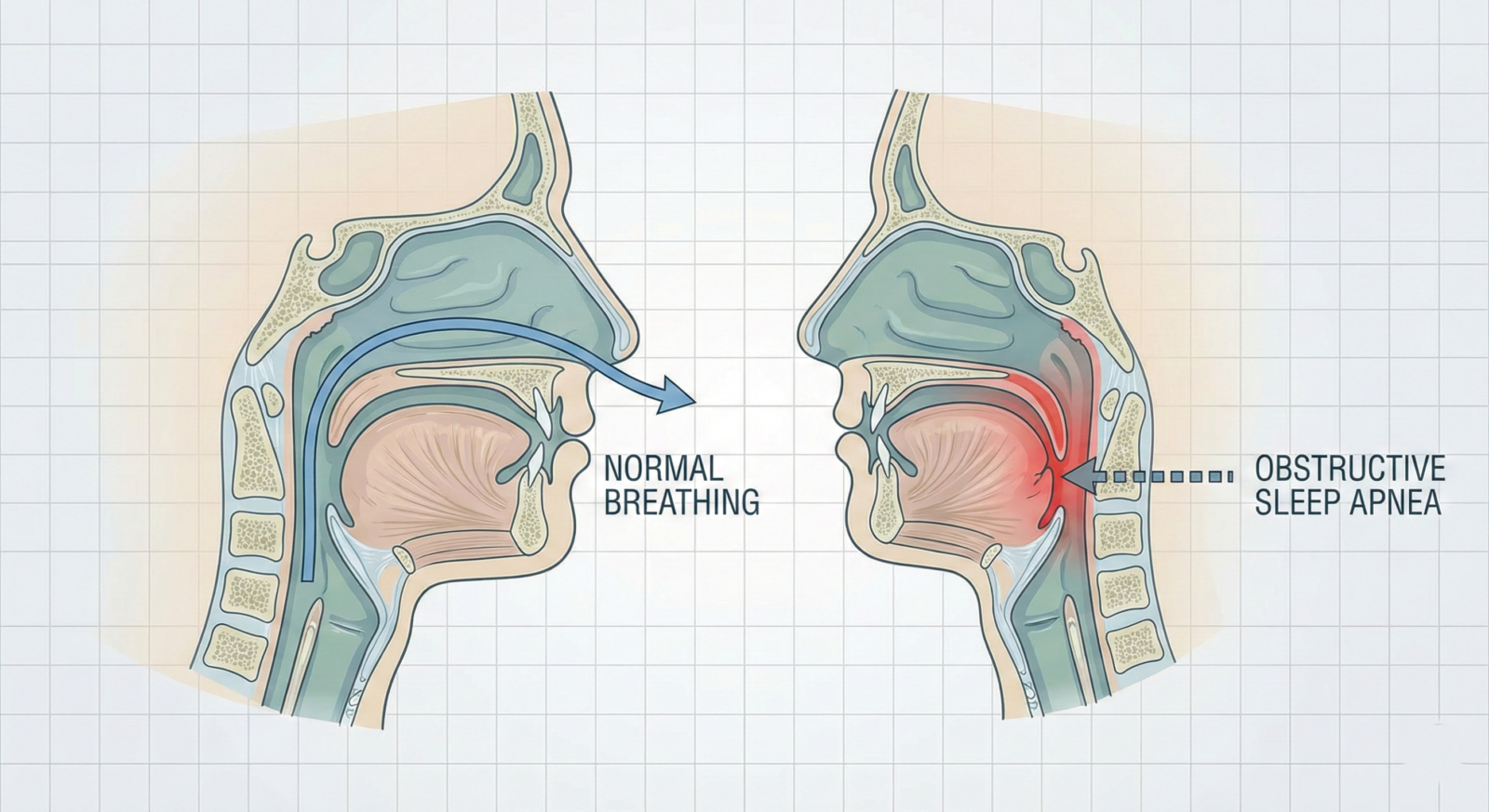
The Mechanics of Obstruction: Why We Stop Breathing
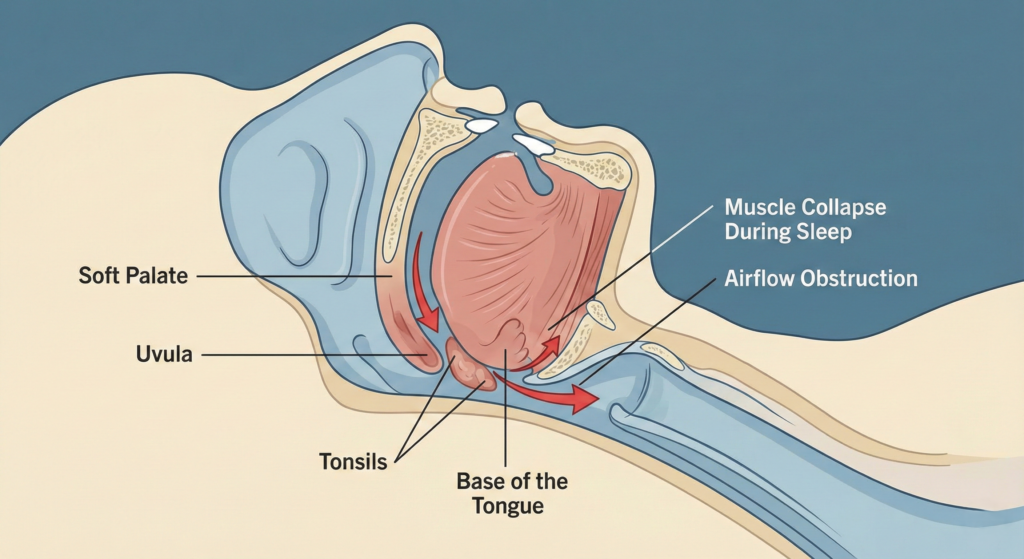
In Obstructive Sleep Apnea, the physical airway is blocked while you sleep, preventing air from reaching your lungs. There are several anatomical and lifestyle factors that trigger this:
- Anatomical Blockages: A deviated septum, enlarged tonsils, or an oversized uvula can physically narrow the passage.
- The “Relaxation” Factor: Alcohol and certain medications (like benzodiazepines) cause the pharyngeal muscles and the tongue to relax and sag backward, closing the airway.
- The “Bull Neck”: Excess weight around the neck (common in obesity) compresses the trachea from the outside when lying down.
The Internal Crisis: Hypoxemia and Hypercapnia
When your airway is blocked, you experience Alveolar Hypoventilation—you aren’t moving enough gas in and out of your lungs. This leads to two dangerous states:
- Hypoxemia: A drop in oxygen levels in the blood.
- Hypercapnia: A buildup of carbon dioxide (CO2).
The critical difference is that in OSA, these events are primarily nocturnal (at night). In OHS, the body struggles with these levels both day and night.
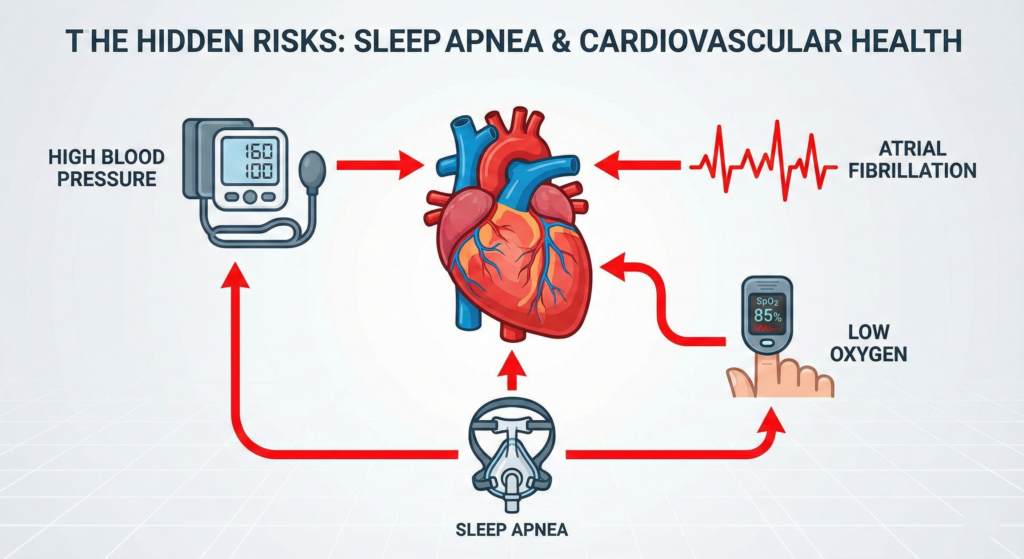
The Danger Zone: Long-term Complications
Living with untreated sleep apnea is not just about being tired; it’s a systemic strain on the body.
- Secondary Hypertension: Low oxygen triggers the sympathetic nervous system, clamping down on arteries and spiking blood pressure.
- Heart Failure: The heart has to work harder against increased resistance in the lungs (pulmonary hypertension), which can lead to right-sided heart failure.
- Atrial Fibrillation (Afib): Hypoxemia can trigger electrical “misfires” in the heart, leading to dangerous irregular rhythms and increased stroke risk.
Diagnosis and Treatment: Taking Control
If you experience daytime somnolence (extreme sleepiness) or your partner witnesses you gasping for air, a Polysomnogram (Sleep Study) is the gold standard for diagnosis.

How is it treated?
- Positive Airway Pressure (CPAP/BiPAP): The most common treatment involves a machine that generates constant pressure to keep your airway “stinted” open while you sleep.
- Weight Loss: Since obesity is a primary driver, weight loss or bariatric surgery can sometimes resolve the condition entirely.
- Surgical Options (UPPP): In cases of severe anatomical obstruction, surgeons can remove excess tissue from the soft palate or tonsils.
- Hypoglossal Nerve Stimulator: A “pacemaker for the tongue” that detects when you breathe and moves the tongue forward to prevent blockage.
Don’t Ignore the Signs
Sleep apnea is a silent thief of health. Whether it’s through simple lifestyle changes or medical intervention, addressing these “pulmonary sleep disorders” is vital for preventing heart disease and improving your quality of life. If you find yourself nodding off during the day, it might be time to talk to a specialist.







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Leave a comment